'Dignity in Silence': Coma, Consciousness, and the Fragility of Life
Reflections on World Coma Day at Johns Hopkins Hospital

“The time has come to realize that an interpretation of the universe—even a positivist one—remains unsatisfying unless it covers the interior as well as the exterior of things; mind as well as matter. The true physics is that which will, one day, achieve the inclusion of man in his wholeness in a coherent picture of the world”
Pierre Teilhard de Chardin. The Phenomenon of Man (1959; pp. 35-36).
Introduction
Some years ago, when I first learned that my wife had been rushed into the emergency room of a local hospital, my mind froze. I found myself struggling to understand how such an event could have occurred without any manifested malaise or known symptom.
The transition triggered by a spontaneous subarachnoid brain hemorrhage was subtle in its onset, but fast in its progression.
As I have narrated before, her life was likely saved by the decision of my second son who was at home at the time to call 911 right away (Marquez 2019). In events such as this, time is critical—every minute can make the difference between life and death (Marquez 2025). The emergency rescue services dispatched an ambulance within minutes and took her to a nearby local hospital. Soon after, my first son, who had rushed to the hospital, called me. I was out on a long Sunday walk when he reached me to share the news and asked me to come to the emergency ward of the hospital right away, saying, “something bad happened to Mom.” When I arrived, my wife had been stabilized and was being prepared for transfer by a medical evacuation helicopter to a specialized tertiary hospital with the capacity to manage such complex cases.
In that moment, I felt torn, suspended, almost in a vacuum, between disbelief and reflection, trying to process what I was hearing and witnessing, while recognizing the need to reframe my thoughts and prepare to confront an unpredictable, fast evolving new reality. It took a few minutes, but contemplation eventually gave way to action. Together with my sons, I called my daughter, who was out of town, so she could arrange her return home that same night. We also began making plans to travel to Baltimore, where the specialized hospital is located, and to find a place to stay nearby.
That day marked the beginning of a journey that would progress over months, moving from crisis to uncertainty, from silence and waiting to small signs of return and recovery, sustained throughout by the unconditional presence of my three children and our extended family, and by a quiet, never-failing faith that “somebody up there likes her.” Indeed, as the days and nights passed, they reinforced a deep belief—one I inherited from my father in the convergence and inseparable connection between science and spirituality.
What has remained with me over the eight years since that experience is not only the memory of fear and a deep sense of uncertainty and vulnerability, but also a more profound realization, an almost existential awakening, of the fragility of life, and how suddenly it can slip into what medicine defines as a coma.
On March 22, the Neurocritical Care Society and the Curing Coma Campaign marks World Coma Day, a global effort to raise awareness about coma, its impact on patients and families, and the need for continued research, care, and support. A timely reminder that behind every case is a human story, and that recovery science matters (Neurocritical Care Society 2026).
Before attending this event at Johns Hopkins Hospital, at the invitation of the Neurosurgery Intensive Care Unit team where my wife was once admitted, I found myself transported back, reliving the experience as I reviewed the literature to better understand the nature of coma: its causes and implications from both biological and human perspectives, and what can be done to support a return toward consciousness and ultimately, to life itself.
Here, in this post, I offer some reflections to help shine a light on this year’s World Coma Day.
Source: Neurocritical Care Society 2026.
What Is Coma?
As described in detail in Figure 1, clinically, coma is defined as a state of profound unresponsiveness in which a patient is alive but unable to wake, respond to stimuli, or engage with the environment, and is characterized by the absence of sleep–wake cycles (Flanagan and Lin 2023). Coma is part of a broader category known as disorders of consciousness (DoC), which also includes the vegetative state and minimally conscious state (Giacino et al. 2018).
This clinical definition, while precise, does not fully capture the lived reality. Coma is not merely the absence of responsiveness, it is a disruption of the complex neural networks that sustain awareness, identity, and connection to others (Edlow et al. 2021).
Recent advances in neuroscience have further complicated our understanding. Evidence suggests that some patients diagnosed as unconscious may retain “covert consciousness” or brain activity indicating awareness that cannot be outwardly expressed (Claassen et al. 2019).
This challenges long-held assumptions and underscores the need for humility in clinical judgment.
Figure 1: Coma Definitions
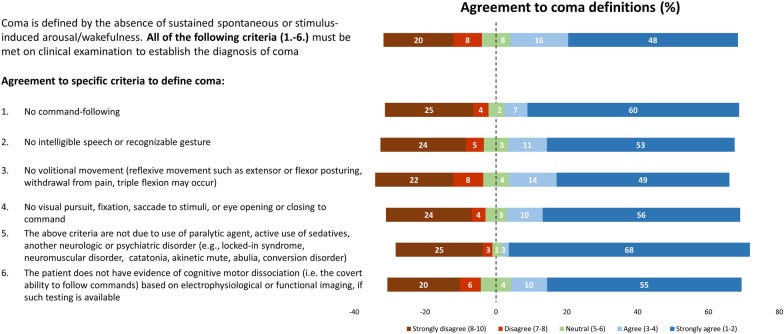
Source: Adapted from Helbok et al. 2022.
Beyond Silence, Covert Consciousness
One of the most important developments in the field over the past decade has been the recognition that consciousness can be present but hidden.
Advanced neuroimaging and electrophysiological techniques and research conducted have demonstrated that some patients who appear entirely unresponsive may, in fact, show brain activation consistent with awareness, a condition often referred to as covert consciousness (Claassen et al. 2019).
At the same time, research findings suggest that misdiagnosis rates may reach up to 30–40%, highlighting the limits of bedside clinical assessment alone (Schnakers et al. 2009).
Uncertainty, therefore, remains a defining feature of coma. As Professor José Ignacio Suárez, a world-class specialist and respected Colombian colleague, who serves as the Chief of the Neurosciences Critical Care Unit at Johns Hopkins Hospital, has observed, such uncertainty affects not only clinicians but especially families seeking answers to the most fundamental question: “Is he or she going to wake up? And, if their loved one does wake up, what will their life look like?” (Walker 2022; Edlow et al. 2021; Tinti et al. 2024).

Source: Photo taken by Giovanni S Marquez, San José de Costa Rica, February 2026.
Causes: When the Brain Is Overwhelmed
Coma is not a disease, but a consequence, a final common pathway of severe brain dysfunction.
Figure 2 lists the most common coma causes. Global evidence indicates that intracerebral hemorrhage, traumatic brain injury, and spontaneous subarachnoid hemorrhage are the leading causes across clinical settings (Helbok et al. 2022).
Figure 2: Coma Etiologies
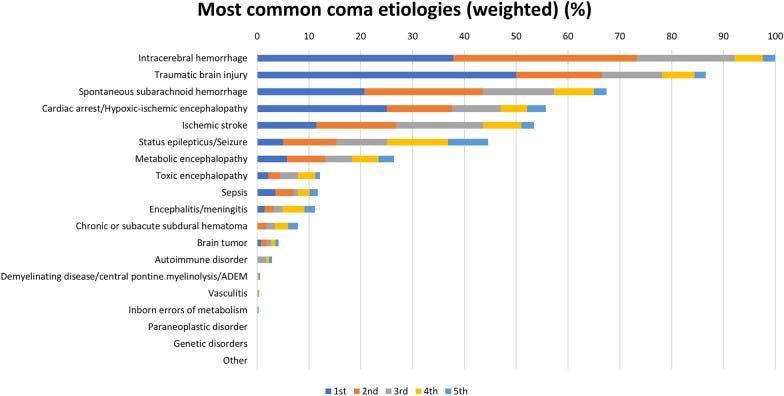
Source: Adapted from Helbok et al. 2022.
Recovery: A Trajectory, Not an Event
One of the most important, and hopeful, insights emerging from recent research is that recovery from coma is not binary (Edlow et al. 2021). That is, it is not a switch from “off” to “on.” It is a trajectory, often slow, nonlinear, and deeply individualized (Giacino et al. 2018; Egawa et al. 2024).
Some patients regain consciousness within days; others show signs of improvement months or even years later. Small behavioral changes, often subtle and easily overlooked, can signal meaningful neurological progress (Giacino et al. 2018).
At the same time, outcomes vary widely. Prognosis depends on factors such as the underlying cause of injury, neurological examination findings, and neuroimaging results, yet it remains inherently uncertain (Helbok et al. 2022).
Studies further show that individuals emerging from prolonged disorders of consciousness often continue to experience significant functional limitations even after one year, underscoring the need for sustained rehabilitation and long-term support (Egawa et al. 2024; Edlow et al. 2021).
Advances in Care: Expanding the Possibility of Recovery
Encouragingly, the field is evolving rapidly (Edlow et al. 2021; Provencio et al. 2020), as highlighted below:
1. Improved Diagnosis
Standardized tools such as the Coma Recovery Scale–Revised (CRS-R) remain the gold standard, while repeated and structured assessments are improving diagnostic accuracy (Giacino et al. 2018; Schnakers et al. 2009).
Emerging technologies are complementing bedside evaluation:
Electroencephalography (EEG) and functional magnetic resonance imaging (fMRI): Measure brain activity through electrical signals and blood flow, respectively, to detect hidden signs of consciousness (Giacino et al. 2018; Claassen et al. 2019; Owen et al. 2006; Monti et al. 2010).
Electromyography-based systems (EMG): Detect subtle muscle activity, helping identify hidden attempts to move or respond (Provencio et al. 2020).
Multimodal diagnostic frameworks: Combine clinical examinations with multiple technologies to improve diagnosis and prognostication (Helbok et al. 2022; Giacino et al. 2018).
Standardized behavioral assessment tools (e.g., Coma Recovery Scale–Revised):
Use structured, repeated evaluations to track levels of consciousness and reduce misdiagnosis (Giacino et al. 2018).
These approaches are increasingly capable of detecting subtle or covert signs of consciousness that may not be evident clinically (Claassen et al. 2019; Edlow et al. 2021).
2. Neurotechnology and Artificial Intelligence
Recent research points toward a future in which AI-assisted monitoring can continuously assess brain function and predict transitions in consciousness states (Edlow et al. 2021).
Machine learning models are already demonstrating the ability to predict coma and delirium trajectories in intensive care unit (ICU) patients with increasing accuracy, offering the potential for earlier and more targeted interventions (Egawa et al. 2024).
3. Neurostimulation and Pharmacologic Therapies
Therapies such as the following are being explored to promote recovery:
Transcranial stimulation: Non-invasive techniques (such as transcranial magnetic or electrical stimulation) that modulate brain activity through the scalp to enhance neural connectivity and promote recovery of consciousness (Thibaut et al. 2014; Lefaucheur et al. 2020).
Deep brain stimulation: An invasive approach in which electrodes are implanted in specific brain regions to deliver targeted electrical impulses, with potential to improve arousal and responsiveness in selected patients (Schiff et al. 2007; Giacino et al. 2018).
Pharmacologic agents (e.g., amantadine): Medications that stimulate brain function or neurotransmitter activity; amantadine has shown evidence of accelerating recovery in some patients with disorders of consciousness (Giacino et al. 2012; Whyte et al. 2005). Among these, amantadine, a dopaminergic and NMDA-receptor modulating agent that enhances arousal, attention, and neural signaling, remains the most widely used neurostimulant in clinical practice, with evidence of benefit in selected patients (Helbok et al. 2022; Giacino et al. 2018). Randomized clinical trial evidence has shown that, in patients with disorders of consciousness following traumatic brain injury, amantadine can accelerate the pace of functional recovery during the subacute phase. While not universally effective, it is currently the best-supported pharmacologic intervention and is recommended in clinical guidelines for carefully selected patients (Giacino et al. 2012; Giacino et al. 2018).
4. Early and Integrated Rehabilitation
Perhaps most importantly, there is growing recognition that recovery depends not only on acute care, but on continuity across the care pathway:
ICU care, where timely stabilization, prevention of secondary brain injury, and adherence to neurocritical care protocols are essential to preserve brain function and create the conditions for potential recovery. Early decisions made in the ICU,, including sedation management, hemodynamic optimization (careful management of a patient’s blood circulation, especially blood pressure, blood flow, and oxygen delivery to ensure adequate perfusion of vital organs, particularly the brain), and avoidance of complications, can significantly influence long-term neurological outcomes (Giacino et al. 2018; Helbok et al. 2022).
Early neurorehabilitation, initiated as soon as the patient is medically stable, has been shown to improve functional outcomes by promoting neuroplasticity, the brain’s ability to adapt, reorganize, and form new neural connections in response to injury, while preventing complications such as contractures (permanent shortening of muscles and joints) and deconditioning (loss of strength and functional capacity due to prolonged immobility), and facilitating the gradual recovery of consciousness and function (Turner-Stokes et al. 2015; World Health Organization 2017).
Long-term community support, including outpatient rehabilitation, social services, and caregiver support systems, which are critical to sustaining recovery, improving quality of life, and addressing the long-term cognitive, emotional, and social consequences experienced by patients and their families (World Health Organization 2022; Provencio et al. 2020).
This aligns closely with broader health system principles: survival must be matched by investment in recovery, function, and quality of life (Edlow et al. 2021; Egawa et al. 2024).
Ethics and Decision-Making Under Uncertainty
Few areas of medicine present more profound ethical challenges.
Prognosis is often uncertain
Clinical assessments may be imperfect
Decisions about life-sustaining treatment carry irreversible consequences
The high rates of misdiagnosis and the emerging evidence of covert consciousness raise a critical concern: That early decisions, made under uncertainty, may inadvertently limit the possibility of recovery (Schnakers et al. 2009; Claassen et al. 2019). Notably, clinical practice varies widely, including when to consider withdrawal of life-sustaining treatment, highlighting the absence of universally accepted standards (Helbok et al. 2022; Yakhkind et al. 2024).
This has led to increasing calls for:
Repeated and standardized assessments, recognizing that recovery of consciousness can be delayed and fluctuating. Serial use of validated tools, such as the Coma Recovery Scale–Revised, helps reduce misdiagnosis and improves detection of subtle signs of awareness over time.
Greater use of advanced diagnostics, including functional MRI, EEG, and other neurophysiological techniques, which can reveal covert consciousness and brain activity not evident on bedside examination alone.
A more cautious and evidence-informed approach to prognostication, avoiding premature or overly deterministic predictions about outcomes, particularly in the early stages after brain injury, when uncertainty remains high and recovery trajectories are variable (Provencio et al. 2020; Suárez 2004).
Building Systems for Recovery: From Acute Care to Long-Term Outcomes
My personal experience, standing in the emergency room and later spending days and nights in a neurosciences critical care unit, confronting the sudden stillness of someone I love, remains a powerful reminder of the fragility of life.
But it also points to a broader challenge. As health systems improve their ability to save lives, they must also strengthen their capacity to restore lives. In many settings, this care is delivered within specialized neurosciences critical care units (NSUs) (Suárez 2004).
The NSUs were developed in response to the recognition that critically ill neurological and neurosurgical patients—across adolescent, adult, and geriatric populations—have distinct and complex needs requiring highly specialized intensive nursing and medical care (Suárez 2004). As such, NSUs are designed as dedicated environments where multidisciplinary teams are equipped to manage the dynamic interplay between systemic physiology and central nervous system function (Suárez 2004).
In turn, the emergence of NSUs has helped shape neurocritical care as a subspecialty, bringing together clinicians from diverse medical and surgical backgrounds. with a shared focus on improving both short- and long-term neurological outcomes (Suárez 2004; Helbok et al. 2022).
Yet strengthening these systems requires more than specialized units alone (Marquez and Chockalingam 2023). It calls for a broader, integrated approach across the continuum of care, within and outside medical facilities:
Investment in neurorehabilitation systems to support functional recovery and long-term outcomes after severe brain injury (World Health Organization 2017; Turner-Stokes et al. 2015).
Adequate financing of services and financial protection mechanisms are essential to ensure equitable access to care across the continuum—from emergency response and intensive care to rehabilitation and long-term support—while protecting patients and families from catastrophic health expenditures and the risk of impoverishment (World Bank Group and World Health Organization 2025; Wagstaff et al. 2018). This includes public financing, insurance coverage, and social protection measures that reduce out-of-pocket costs and financial hardship.
Support for families and caregivers, who experience significant psychological, social, and economic burdens when caring for individuals with disorders of consciousness (Provencio et al. 2020; Helbok et al. 2022).
Integration of mental health and psychosocial care into recovery pathways, recognizing the emotional and cognitive sequelae affecting both patients and caregivers (World Health Organization 2022; Marquez 2023; Giacino et al. 2018).
Strengthening of multidisciplinary care models, including neurosciences critical care units and coordinated post-acute services, to ensure that expertise, technology, and human-centered care are aligned across the continuum of care (Suárez 2004; World Health Organization 2017; Helbok et al. 2022).
Continued investment in research and innovation, including advances in neuroimaging, biomarkers, and therapeutic interventions aimed at improving diagnosis, prognostication, and recovery (Edlow et al. 2021; Egawa et al. 2024).
Global evidence shows significant variability in coma care across settings—highlighting the need for coordinated, evidence-based systems that extend from emergency response to acute care and long-term recovery, anchored in universal health coverage arrangements that ensure individuals and families can access needed services without suffering financial hardship (Helbok et al. 2022; Provencio et al. 2020; World Bank Group and World Health Organization 2025).
In many ways, therefore, disorders of consciousness sit at the intersection of medicine, neuroscience, ethics, and public health.

Source: Image id Shutterstock_1878018001 (1)

Source: Adapted from Forty Years of Neurocritical Care | Johns Hopkins Medicine

Source: The JHH Neurosciences Critical Care Unit (NCCU) Team, Adapted from Forty Years of Neurocritical Care | Johns Hopkins Medicine
Closing Reflection
As I attend today this World Coma Day event at Johns Hopkins Hospital, I do so not only as a public health practitioner, but as someone who has witnessed firsthand the fragile boundary between presence and absence.
Coma is not simply a medical condition. It is a threshold—between silence and awareness, between uncertainty and possibility. And increasingly, as discussed above, science is teaching us that even in that ‘dignified silence’, something may remain—waiting, perhaps, for the conditions that allow it to return.
In reflecting on this journey, both personal and collective, I am reminded of the timeless words of Pedro Calderón de la Barca (1635) in the classical Spanish play, La vida es sueño:
¿Qué es la vida? Un frenesí.
¿Qué es la vida? Una ilusión,
una sombra, una ficción,
y el mayor bien es pequeño:
que toda la vida es sueño,
y los sueños, sueños son.
(*What is life? A frenzy.
What is life? An illusion,
a shadow, a fiction;
and the greatest good is but small:
for all of life is a dream,
and dreams are but dreams.)
Perhaps nowhere does this reflection resonate more deeply than in the experience of coma, where life itself seems suspended between dream and reality, between absence and return.
And yet, within that fragile space, there remains not only uncertainty, but also the enduring possibility of recovery, connection, and life reclaimed.
References
Calderón de la Barca, Pedro. 1635. La vida es sueño. Biblioteca Virtual Miguel de Cervantes. https://www.cervantesvirtual.com/obra-visor/la-vida-es-sueno--0/html/fedc73fa-82b1-11df-acc7-002185ce6064_2.html#I_0_
Claassen, Jan, Katherine Doyle, A. Matory, Yelena G. Bodien, et al. 2019.
“Detection of Brain Activation in Unresponsive Patients with Acute Brain Injury.” New England Journal of Medicine 380 (26): 2497–2505.
https://doi.org/10.1056/NEJMoa1812757
Edlow, Brian L., Jan Claassen, Nicholas D. Schiff, and David M. Greer. 2021.
“Recovery from Disorders of Consciousness: Mechanisms, Prognosis and Emerging Therapies.” Nature Reviews Neurology 17 (3): 135–156.
https://doi.org/10.1038/s41582-020-00428-x
Egawa, Satoshi, Jeremy Ader, and Jan Claassen. 2024.
“Recovery of Consciousness after Acute Brain Injury: A Narrative Review.” Journal of Intensive Care 12 (1): 37.
https://doi.org/10.1186/s40560-024-00749-9
Flanagan, Steven, and Jing Lin. 2023. “Disorders of Consciousness.” AAPM&R Knowledge NOW.
https://now.aapmr.org/disorders-of-consciousness/
Giacino, Joseph T., John Whyte, Emilia Bagiella, Kathleen Kalmar, et al. 2012.
“Placebo-Controlled Trial of Amantadine for Severe Traumatic Brain Injury.” New England Journal of Medicine 366 (9): 819–826.
https://doi.org/10.1056/NEJMoa1102609
Giacino, Joseph T., Douglas I. Katz, Nicholas D. Schiff, John Whyte, Eric J. Ashman, Stephen Ashwal, Richard Barbano, et al. 2018.
“Practice Guideline Update Recommendations Summary: Disorders of Consciousness.” Neurology 91 (10): 450–460.
https://doi.org/10.1212/WNL.0000000000005926
Helbok, Raimund, Vicki Rass, Ettore Beghi, Yelena G. Bodien, Giuseppe Citerio, Joseph T. Giacino, Daniel Kondziella, et al. 2022. “The Curing Coma Campaign International Survey on Coma Epidemiology, Evaluation, and Therapy (COME TOGETHER).” Neurocritical Care 37 (1): 47–59.
https://doi.org/10.1007/s12028-021-01425-8
Lefaucheur, Jean-Pascal, André Aleman, Chris Baeken, et al. 2020.
“Evidence-Based Guidelines on the Therapeutic Use of Repetitive Transcranial Magnetic Stimulation (rTMS): An Update (2014–2018).” Clinical Neurophysiology 131 (2): 474–528. https://doi.org/10.1016/j.clinph.2019.11.002
Marquez, Patricio V. 2019. “A personal perspective from the medical care frontlines”. World Bank Blogs, Investing in Health, January 7, 2019. https://blogs.worldbank.org/en/health/personal-perspective-medical-care-frontlines
Marquez, Patricio V. 2023. “Mental Health Is as Important as Physical Health in a Post-Pandemic World.” Substack post, October 24, 2025 (originally published January 21, 2023). https://open.substack.com/pub/pmarquez/p/mental-health-is-as-important-as?utm_campaign=post-expanded-share&utm_medium=web
Marquez, Patricio V. 2025. “Improving Road Safety: The Critical Role of Post-Crash Care in Saving Lives and Preventing Serious Disability.” Substack Post, February 23, 2025. https://open.substack.com/pub/pmarquez/p/improving-road-safety-the-critical?utm_campaign=post-expanded-share&utm_medium=web
Marquez, Patricio V., and Arun Chockalingam. 2023. “Public Health Practice—A Futuristic Perspective.” In Principles and Application of Evidence-Based Public Health Practice, edited by Soundappan Kathirvel, Amarjeet Singh, and Arun Chockalingam, 287–322. Elsevier. https://doi.org/10.1016/B978-0-323-95356-6.00008-2
Monti, Martin M., Audrey Vanhaudenhuyse, Martin R. Coleman, Melanie Boly, John D. Pickard, Steven Laureys, and Adrian M. Owen. 2010.
“Willful Modulation of Brain Activity in Disorders of Consciousness.” New England Journal of Medicine 362 (7): 579–589.
https://doi.org/10.1056/NEJMoa0905370
Neurocritical Care Society. 2026. “World Coma Day.” https://www.neurocriticalcare.org/Events/Event-Calendar/Event-Details/world-coma-day
Owen, Adrian M., Martin R. Coleman, Melanie Boly, Matthew H. Davis, Steven Laureys, and John D. Pickard. 2006. “Detecting Awareness in the Vegetative State.” Science 313 (5792): 1402. https://doi.org/10.1126/science.1130197
Provencio, J. Javier, J. Claude Hemphill III, Jan Claassen, Brian L. Edlow, Raimund Helbok, Daniel Kondziella, Nicholas D. Schiff, José I. Suárez, et al. 2020.
“The Curing Coma Campaign: Framing Initial Scientific Challenges—Proceedings of the First Curing Coma Campaign Scientific Advisory Council Meeting.” Neurocritical Care 33 (1): 1–12. https://doi.org/10.1007/s12028-020-01028-9
Schnakers, Caroline, Audrey Vanhaudenhuyse, Joseph T. Giacino, Marie-Aurélie Ventura, Mélanie Boly, Steven Laureys, et al. 2009. “Diagnostic Accuracy of the Vegetative and Minimally Conscious State: Clinical Consensus versus Standardized Neurobehavioral Assessment.” BMC Neurology 9: 35. https://doi.org/10.1186/1471-2377-9-35
Schiff, Nicholas D., Joseph T. Giacino, Kathleen Kalmar, Jeffrey D. Victor, Michael Baker, Daniel J. Gerber, Beth Fritz, et al. 2007. “Behavioural Improvements with Thalamic Stimulation after Severe Traumatic Brain Injury.” Nature 448 (7153): 600–603. https://doi.org/10.1038/nature06041
Suárez, José I., ed. 2004. Critical Care Neurology and Neurosurgery. Totowa, NJ: Humana Press. https://doi.org/10.1007/978-1-59259-660-7
Teilhard de Chardin, Pierre. 1959. The Phenomenon of Man. Translated by Bernard Wall. Reprint, New York: Harper Perennial Modern Classics, 2008, pp.35-36. https://www.harpercollins.com/products/the-phenomenon-of-man-pierre-teilhard-de-chardin?variant=32131128885282
Thibaut, Aurore, Athena Bruno, Olivia Ledoux, Steven Laureys, and Audrey Vanhaudenhuyse. 2014. “tDCS in Patients with Disorders of Consciousness: Sham-Controlled Randomized Double-Blind Study.” Neurology 82 (13): 1112–1118.
https://doi.org/10.1212/WNL.0000000000000260
Tinti, Lorenzo, Thomas Lawson, Erika Molteni, Daniel Kondziella, Verena Rass, Tarek Sharshar, Yelena G. Bodien, et al. 2024. “Research Considerations for Prospective Studies of Patients with Coma and Disorders of Consciousness.” Brain Communications 6 (1): fcae022. https://doi.org/10.1093/braincomms/fcae022
Turner-Stokes, Lynne, Peter B. Disler, Ajoy Nair, and Derick T. Wade. 2015.
“Multi-Disciplinary Rehabilitation for Acquired Brain Injury in Adults of Working Age.” Cochrane Database of Systematic Reviews, no. 12: CD004170.
https://doi.org/10.1002/14651858.CD004170.pub3
Wagstaff, Adam, et al. 2018. “Progress on Catastrophic Health Spending in 133 Countries.” Lancet Glob Health: 6: e169–79. https://openknowledge.worldbank.org/entities/publication/41e69b62-0008-5e7f-9d5c-85d028d46ad8
Walker, Cameron. 2022. “A Cure for Coma? Advances in Research and Care.” Johns Hopkins Magazine. https://hub.jhu.edu/magazine/2022/fall/coma-cure-research/
Whyte, John, Douglas I. Katz, David Long, Annette M. DiPasquale, David Polansky, Nancy L. Kalmar, Tessa Hart, et al. 2005.
“Predictors of Outcome in Prolonged Posttraumatic Disorders of Consciousness and Assessment of Medication Effects: A Multicenter Study.” Archives of Physical Medicine and Rehabilitation 86 (3): 453–462.
https://doi.org/10.1016/j.apmr.2004.05.016
World Bank Group and World Health Organization. 2025.
Tracking Universal Health Coverage: 2025 Global Monitoring Report.
https://www.worldbank.org/en/topic/universalhealthcoverage/publication/2025-global-monitoring-report-gmr
World Health Organization. 2017. Rehabilitation in Health Systems. Geneva: WHO.
https://www.who.int/publications/i/item/9789241549974
World Health Organization. 2022. World Mental Health Report: Transforming Mental Health for All. Geneva: WHO. https://www.who.int/publications/i/item/9789240049338
Yakhkind, Aleksandra, Naomi Niznick, Yelena G. Bodien, Flora M. Hammond, Douglas Katz, Jacques Luaute, Molly McNett, Lionel Naccache, Katherine O’Brien, Caroline Schnakers, Thierry Sharshar, Beth S. Slomine, Joseph T. Giacino, and the Curing Coma Campaign. 2024. “Common Data Elements for Disorders of Consciousness: Recommendations from the Working Group on Behavioral Phenotyping.” Neurocritical Care 40 (3): 909–917. https://doi.org/10.1007/s12028-023-01844-9
